In simpler videolaparoscopic procedures, such as cholecystectomy and uncomplicated appendectomies, robotic surgery adds little to the advantage,
since these procedures are very easily performed by the conventional videolaparoscopic method.
However, we have routinely used the robot in some less complex procedures such as correction of gastroesophageal reflux, correction of inguinal
hernias and other hernias of the abdominal wall.
The biggest advantage in using robotic surgery occurs in the most complex procedures. In the field of general surgery and the digestive tract, the procedure
s that benefit most from this method are pancreas, liver and biliary tract surgeries.
Since 2018, we have been using the robot in all these surgeries instead of laparoscopy. With this, we were able to increase the proportion of patients who benefit
from the minimally invasive method, because in some situations where the use of laparoscopy was not possible and we needed the use of open surgery, today with the robot this is not only possible but also desired.
An example of this is its use in Klatskin³ tumors, that is, hilar cholangiocarcinoma³. Another important example is its use in pancreatic cancer.
Surgeries such as pancreaticoduodenectomy4 or Whipple surgery4 are routinely performed by our team robotically today.
In cases with vascular invasion, previously a contraindication regarding the use of laparoscopy, the use of the robot facilitates its safe performance in
selected cases.
Another frequent use of the robot occurs in patients who have already undergone multiple open surgeries, where most surgeons in the world contraindicate
minimally invasive surgery due to the presence of adhesions. Robotic surgery helps a lot in the release of adhesions and thus, we are able to perform
surgeries, even complex ones, in these patients.
The use of the robot in this situation will provide a better postoperative result, as well as allow further surgeries to continue to be performed by a
minimally invasive route, as once adhesions are released using this technique, they do not form again with the same intensity. A liver surgery5
in this extreme situation was the subject of a publication in an international journal5.
Another important use is in complex bile duct surgeries such as in cases with bile duct stenosis (narrowing) caused by accidental injuries during previous surgeries or by other causes. A bile duct surgery in this extreme situation was the subject of one of our publications in an international journal6.
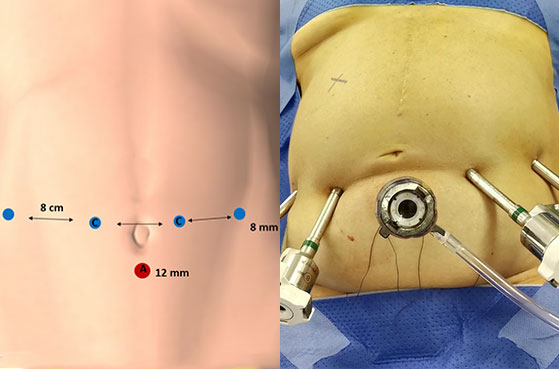
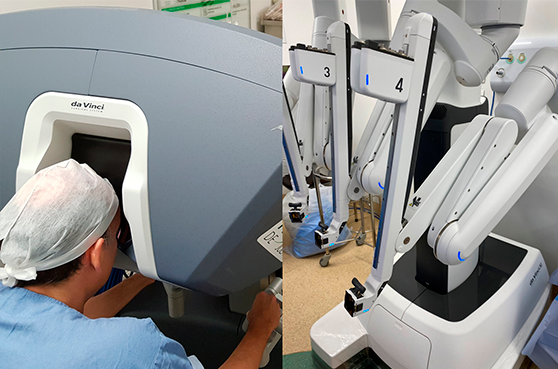
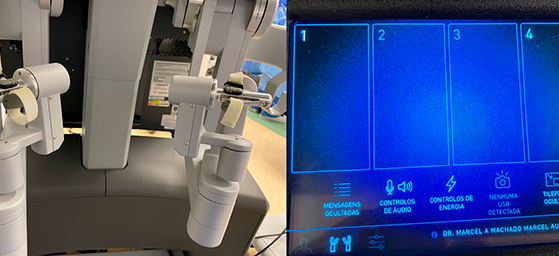
How is robotic surgery performed? Through small incisions (Image 1), through which the trocars enter (cannulas through which the different robotic forceps, optics and other instruments enter). The robot uses 4 trocars. An extra trocar is used by the assistant surgeon to introduce sutures, aspirator, stapler, etc. (Image 1). The surgeon is on a console (Image 2) from where he commands the movement of the 4 robot arms (camera and 3 tweezers). (Images 3 and 4). Video 1 shows how the robotic system works.
- 1 – 063 Robotic liver resection. Report of pioneering experience in Latin America
- 2 – 135 Robotic Resection of Intraductal Neoplasm of the Pancreas
- 3 – 215 Robotic Resection of Hilar Cholangiocarcinoma
- 4 – 200 Robotic pancreaticoduodenectomy after Roux-en-Y gastric bypass
- 5 – 198 Robotic Repeat Right Hepatectomy for Recurrent Colorectal Liver Metastasis
- 6 – 203 Robotic Left Hepatectomy and Roux-en-Y Hepaticojejunostomy
Schedule your appointment